For the treatment of portal hypertension, it is advisable to use. What is portal hypertension syndrome - symptoms, manifestations and treatment of the disease
a common part
Portal hypertension is a syndrome of increased pressure in the portal vein system caused by impaired blood flow in the portal vessels, hepatic veins and inferior vena cava.
Portal hypertension is accompanied by splenomegaly (enlargement of the spleen), varicose veins of the esophagus and stomach, ascites, hepatic encephalopathy (liver failure).
Normally, the pressure in the portal vein system is 5-10 mm Hg. Increased pressure in the portal vein system above 12 mm Hg. indicates the development of portal hypertension.
Varicose veins occur when the pressure in the portal system is more than 12 mm Hg. Art.
In most cases, portal hypertension is a consequence of liver cirrhosis, schistosomiasis (in endemic areas), structural abnormalities of the hepatic vessels.
If, with portal hypertension, the pressure in the small hepatic vein is greater than or equal to 12 mm Hg. Art., between the portal system and the systemic venous network, collateral circulation occurs. Collaterals (varicose veins) divert part of the portal blood flow from the liver, which helps to reduce portal hypertension, but never completely eliminates it. Collaterals arise in places of close location of the branches of the portal and systemic venous network: in the mucous membrane of the esophagus, stomach, rectum; on the anterior abdominal wall (between the umbilical and epigastric veins).
The portal system of the liver.
The diagnosis of portal hypertension is based on clinical evaluation, imaging, and endoscopy.
Treatment consists in medical and endoscopic measures aimed at preventing bleeding from the dilated veins of the esophagus, stomach, intestines. Surgical methods of therapy include portosystemic shunting.
- Epidemiology of portal hypertension
There are no precise quantitative data on the incidence of portal hypertension.
In 90% of patients with liver cirrhosis, varicose veins of the esophagus, stomach and intestines occur. In 30% of cases, it is complicated by bleeding. Mortality after the first episode of bleeding is 30-50%. In 70% of patients who survived one episode of bleeding from varicose veins of the esophagus, bleeding occurs repeatedly.
Among all the causes of gastrointestinal bleeding, varicose veins of the esophagus and stomach account for 5-10%. The risk of this complication is highest in patients with portal hypertension caused by splenic vein thrombosis.
- Etiology of portal hypertension
- Causes of prehepatic portal hypertension
- Portal vein thrombosis.
- Splenic vein thrombosis.
- Congenital atresia or stenosis of the portal vein.
- Compression of the portal vein by tumors.
- Increased blood flow in the portal vein with arteriovenous fistulas, significant splenomegaly, hematological diseases.
- Reasons for the development of intrahepatic portal hypertension
- The reasons for the development of presinusoidal portal hypertension:
- Schistosomiasis (initial stage).
- Primary biliary cirrhosis (initial stage).
- Sarcoidosis
- Tuberculosis.
- Idiopathic portal hypertension (initial stage).
- Nodular regenerative hyperplasia due to obliterating venopathy.
- Myeloproliferative diseases.
- Polycystic disease.
- Liver metastases.
- The reasons for the development of sinusoidal portal hypertension:
- Cirrhosis of the liver.
- Acute alcoholic hepatitis.
- Acute fulminant hepatitis.
- Pelious hepatitis.
- Congenital liver fibrosis.
- Schistosomiasis (late stage).
- Primary biliary cirrhosis (late stage).
- Idiopathic portal hypertension (late stage).
- The reasons for the development of post-sinusoidal portal hypertension:
- Veno-occlusive disease.
- Non-cirrhotic portal fibrosis of the liver caused by prolonged intake of large doses (3 or more times higher than recommended) of vitamin A.
- With cirrhosis of the liver, chronic active hepatitis, portal hypertension is of a mixed nature: sinusoidal and postsinusoidal; with primary biliary cirrhosis - presinusoidal and postsinusoidal.
- The reasons for the development of presinusoidal portal hypertension:
- Reasons for the development of posthepatic portal hypertension
- Hepatic vein thrombosis (Budd-Chiari syndrome).
- Obstruction of the inferior vena cava.
- Right ventricular heart failure caused by constrictive pericarditis, restrictive cardiomyopathy.
- Arterial portal venous fistula.
- Increased blood flow in the portal vein system.
- Increased blood flow to the spleen.
- Causes of prehepatic portal hypertension
- Pathogenesis of portal hypertension
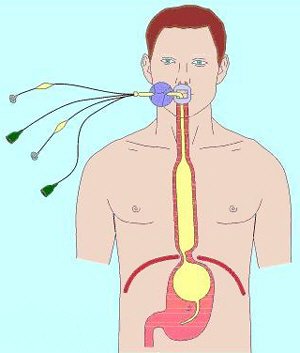
Blood enters the liver through the portal vein system and the hepatic artery. The portal vein receives blood from the superior mesenteric and splenic veins, which collect it from the digestive tract, spleen and pancreas.


The figures show a diagram of the outflow of venous blood from the gastrointestinal tract into the portal system.
Both streams (venous and arterial) are connected in the liver at the level of sinusoids.
In the sinusoids, mixed portal and arterial blood comes into contact with the microvilli of hepatocytes in the Disse spaces, which ensures that the liver performs metabolic functions. Normally, the pressure in the portal vein system is 5-10 mm Hg.

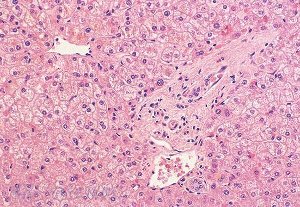
Microscopic structure of liver tissue: 1 - hepatocytes; 2 - terminal hepatic venule; 3 - liver sinusoids.
An increase in pressure in the portal vein system indicates the development of portal hypertension. Portal hypertension is a consequence of increasing pressure in the portal vein or in one of its branches (physiological portal pressure reaches a maximum of 7-12 mm Hg), which is caused both by an increase in venous resistance in the prehepatic, hepatic and posthepatic parts of the portal system, and abdominal blood flow. This occurs against the background of a decrease in arterial vascular resistance.
Portal hypertension is a consequence of liver cirrhosis, schistosomiasis (in endemic areas), structural abnormalities of the hepatic vessels.
With cirrhosis of the liver, a characteristic symptom complex develops - portal hypertension syndrome, caused by a significant increase in pressure in the vein system, which provides blood flow from most organs located in the abdominal cavity to the liver.
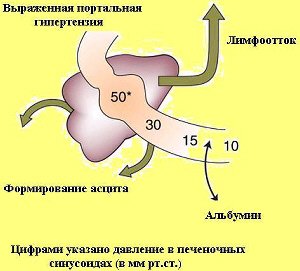
With cirrhosis of the liver, the affected liver is not able to pass through itself the amount of fluid, the transit of which was provided by a healthy liver under normal conditions. A certain amount of the liquid part of the blood is “squeezed out” through the venous wall and penetrates into the surrounding tissues, and later can enter the abdominal cavity.
An increase in pressure in the portal vein is accompanied by an increased release of fluid into the lymphatic bed. As a result, the lymphatic vessels expand significantly.
However, in the pathogenesis of ascites, the decisive role belongs not to the violation of patency in the portal vein system, but to the difficulties of blood and lymph outflow at the level of the hepatic lobules. In cirrhosis, structural changes in the liver are observed: the progressive deposition of collagen and the formation of regeneration nodes disrupt the normal architectonics of the liver and increase the resistance to portal blood flow. Sinusoids become less stretchable due to the accumulation of collagen in the Disse space.
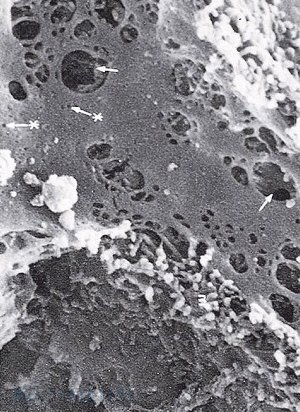
Hepatic sinusoids represent a specific capillary bed. Sinusoidal endothelial cells form a membrane with many pores (indicated by arrows), almost completely permeable to macromolecules, including plasma proteins.
The pore size of the internal capillaries is 50-100 times smaller than that of the hepatic sinusoids, therefore the gradient of the transsinusoidal oncotic pressure in the liver is almost zero, while in the hepatic circulation it is 0.8-0.9. The high oncotic pressure gradient minimizes the effect of any changes in plasma albumin concentration on transmicrovascular fluid exchange.

Portal hypertension increases the hydrostatic pressure in the liver sinusoids.
In the later stages of liver cirrhosis, the pores in the endothelium of the sinusoids disappear, and its permeability decreases. There is a pressure gradient between the interstitial spaces of hepatocytes and the lumen of the sinusoids.
In healthy people, almost 100% of the blood passing through the portal vein system (portal blood flow rate of about 1 L / min) enters the hepatic vein. In a patient with cirrhosis, this figure is 87%. Portal hypertension develops. This is facilitated by systemic vasodilation and a decrease in vascular fertility.
If, with portal hypertension, the pressure in the small hepatic vein is greater than or equal to 12 mm Hg. Art., between the portal system and the systemic venous network, collateral circulation occurs. Collaterals arise in places of close location of the branches of the portal and systemic venous network: in the mucous membrane of the esophagus, stomach (portal hypertensive gastropathy), rectum; on the anterior abdominal wall between the umbilical and epigastric veins (on the anterior abdominal wall in patients with this pathology, a "jellyfish head" is visualized).
Collaterals (varicose veins) divert part of the portal blood flow from the liver, which helps to reduce portal hypertension, but never completely eliminates it. The most common occurrence of varicose veins occurs in the esophagus and stomach.

The scheme of the liver blood circulation and the mechanism of development of portal hypertension and varicose veins of the esophagus.
Bleeding results from varicose veins in the esophagus, stomach and intestines.
The consequences of portal hypertension are the development of portocaval anastomoses, ascites and splenomegaly, often with symptoms of hypersplenism.
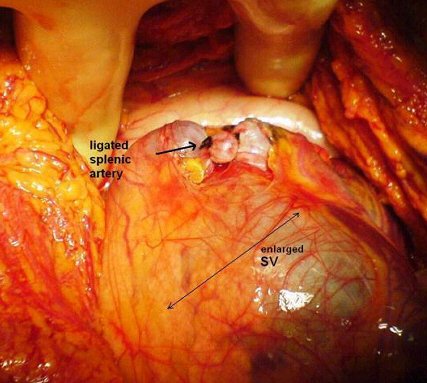
Gradually, patients with portal hypertension develop extrahepatic portosystemic shunts. Blood from the digestive tract enters the systemic circulation, bypassing the liver. Overflow of blood to internal organs contributes to the onset of ascites. Splenomegaly and hypersplenism phenomena (thrombocytopenia, leukopenia, anemia) result from increased pressure in the splenic vein.

- Diagnosis of portal hypertension
Portal hypertension in a patient with chronic liver disease can be suspected by the presence of collateral circulation, splenomegaly, ascites, and hepatic encephalopathy.
- The goals of diagnosing portal hypertension
- Diagnosis of portal hypertension and assessment of the severity.
- Establishing the localization of the portal circulation block.
- Assessment of the risk of complications.
- Diagnostic methods for portal hypertension
- Taking anamnesis
In the course of collecting anamnesis, information can be obtained about the cause of portal hypertension. For this purpose, the fact that the patient has a chronic liver disease is established. Suspicion of cirrhosis of the liver may arise if the patient has a long-term alcohol abuse, a history of viral (B or C) or autoimmune hepatitis.
If schistosomiasis is suspected, it is necessary to find out whether the patient has been in countries where this disease is common. These include: Egypt, Greece, China, Portugal, Cyprus. It is important to remember that the most severe complication of schistosomiasis is periportal fibrosis with the development of portal hypertension, which can occur 10-15 years after infection with Schistosoma mansoni.
If there is a suspicion of congenital liver fibrosis, then it must be remembered that its clinical manifestations in 75% of patients occur at the age of 2-14 years; 15% - at the age of 15-25; 10% - at the age of 25. The disease is hereditary, therefore, liver fibrosis can also be detected in the patient's relatives. The causes of congenital liver fibrosis are: alpha1-antitrypsin deficiency; Wilson-Konovalov disease; fructosemia; galactosemia; glycogenosis (types III, IV, VI, IX and X), hemochromatosis, tyrosinemia, Budd-Chiari syndrome.
Liver damage can be caused by taking certain medications (amiodarone, chlorpromazine, isoniazid, methotrexate, methyldopa, tolbutamide); exposure to toxins (arsenic, iron, copper).
When collecting anamnesis, you can also suspect the presence of complications in the patient. To this end, it is important to find out if the patient had vomiting with blood or melena (may indicate bleeding from varicose veins of the esophagus or stomach), bloody stools (with bleeding from varicose veins of the rectum).
If you suspect the development of hepatic encephalopathy, it is necessary to assess the mental status of the patient (whether there is increased drowsiness, irritability).
With the formation of ascites, the patient can draw the doctor's attention to a noticeable increase in the volume of the abdomen.
It is important to ask the patient if he has had a fever and abdominal pain, as often spontaneous bacterial peritonitis can be almost asymptomatic.
- Physical examination
In the initial, compensated phase, portal hypertension is clinically not manifested or manifested by nonspecific dyspeptic disorders - flatulence, a tendency to diarrhea, nausea and pain in the upper abdomen, more often in the epigastric region.
The stage of decompensated, or complicated, portal hypertension is characterized by the development of one or more often several symptoms: significant cytopenia (hypersplenism), pronounced varicose veins of the esophagus and stomach, the appearance of edematous-ascitic syndrome and encephalopathy.
Physical examination reveals signs of collateral circulation, manifestations of chronic liver disease, symptoms of hypervolemia:
- Signs of collateral circulation:
- Expansion of the veins of the anterior abdominal wall.
- "Medusa's head" (convoluted vessels around the navel).
- Expansion of hemorrhoidal veins.
- Ascites.
- Peri-umbilical hernia.
- Signs of chronic liver disease:
- Jaundice.
- Vascular asterisks.
- Palmar erythema.
- Tremor.
- Gynecomastia.
- Testicular atrophy.
- Splenomegaly.
- Muscular wasting.
- Dupuytren's contracture.
- Signs of hemodynamic disturbances, indicating hypervolemia:
- Arterial hypotension.
- Warm limbs.
- Pulse of good filling.
- Signs of collateral circulation:
- Laboratory research methods
Laboratory research methods are carried out to diagnose diseases that led to liver cirrhosis, which is the most common cause of portal hypertension.
- Clinical blood test.
In patients with liver cirrhosis, a decrease in the number of platelets is observed. The development of anemia or other cytopenias is observed in the later stages of the disease. With hypersplenism, pancytopenia develops (anemia, leukopenia, thrombocytopenia).
For patients with hemochromatosis, a combination of high hemoglobin content with low hemoglobin concentration in erythrocytes is characteristic.
- Coagulogram.
In patients with liver cirrhosis, a decrease in the prothrombin index is observed (the ratio of the standard prothrombin time to the prothrombin time in the patient being examined, expressed as a percentage). Reference values: 78 - 142%.
Prothrombin time (sec) reflects the clotting time of plasma after adding thromboplastin-calcium mixture. Normally, this figure is 15-20 seconds.
- Blood chemistry.
Biochemical liver samples may not differ from normal values \u200b\u200beven with pronounced portal hypertension.
In the biochemical analysis of the blood of patients with liver cirrhosis, it is necessary to determine the following parameters: alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), gamma-glutamyl transpeptidase (GGTP), bilirubin, albumin, potassium, sodium, creatinine.
With compensated cirrhosis of the liver, the activity of liver enzymes may be normal. A significant increase in ALT, ASAT, GGTP is observed in alcoholic hepatitis with an outcome in cirrhosis, and a sharp increase in alkaline phosphatase in primary biliary cirrhosis. In addition, in patients with liver cirrhosis, total bilirubin increases, and albumin content decreases. The content of aminotransferases in the terminal stage of liver cirrhosis always decreases (there are no functioning hepatocytes and no enzymes).
Indicators of unfavorable prognosis: bilirubin is above 300 μmol / l; albumin below 20 g / l; prothrombin index less than 60%.
In patients with edematous-ascites syndrome, it is necessary to determine the content of electrolytes, albumin, urea, creatinine in the blood.
- Determination of antibodies to chronic hepatitis viruses.
Antibodies to viruses that cause chronic hepatitis should be investigated, even if cirrhosis of the liver is directly related to chronic alcohol intoxication.
- Diagnostics of viral hepatitis B (HBV).
The main marker is HbsAg, HBV DNA. The presence of HBeAg indicates viral replication activity. The disappearance of HBeAg and the appearance of antibodies to it (anti-HBe) characterize the termination of HBV replication and is interpreted as a state of partial seroconversion. There is a direct relationship between the activity of chronic viral hepatitis B and the presence of viral replication and vice versa.
- Diagnostics of viral hepatitis C (HCV).
The main marker is antibodies to HCV (anti-HCV). The presence of a current infection is confirmed by detection of HCV RNA. Anti-HCV is detected in the convalescent phase and ceases to be detected 1-4 years after acute viral hepatitis. An increase in these indicators indicates chronic hepatitis.
- Diagnostics of viral hepatitis B (HBV).
- Determination of levels of IgA, IgM, IgG in blood serum.
Elevated levels of serum IgA, IgM, IgG are often detected in alcoholic liver damage, primary biliary cirrhosis and autoimmune diseases, but they do not always change regularly during treatment, and therefore the results of these studies are difficult to evaluate in some cases.
- Urine tests.
In liver cirrhosis, it is important to determine the parameters characterizing renal function (protein, leukocytes, erythrocytes, creatinine, uric acid). This is important, since in 57% of patients with liver cirrhosis and ascites, renal failure is detected (endogenous creatinine clearance less than 32 ml / min with normal serum creatinine levels).
In patients with edematous-ascites syndrome, it is necessary to determine the daily urine output.
- Clinical blood test.
- Instrumental diagnostic methods




- Magnetic resonance imaging
Magnetic resonance imaging allows you to obtain an image of the parenchymal organs of the abdominal cavity, large vessels, and retroperitoneal space.
With this method, you can diagnose diseases of the liver and other organs; determine the level of portal circulation blockade and the severity of collateral blood flow; the condition of the veins of the liver and the presence of ascites; to evaluate the function of the splenorenal anastomosis after surgical treatment.
- Hepatoscintigraphy
This study makes it possible to determine (by the distribution of the pharmaceutical preparation) the absorption-excretory function of the liver, its size and structure. You can assess the severity of cirrhotic changes in the liver.
In addition, in portal hypertension, radioisotope drugs accumulate not only in the liver, but also in the spleen.



- Splenomanometry
Splenomanometry is used to establish the form of portal hypertension, determine the pressure in the portal system and assess the state of the vascular bed.
For this purpose, a spleen puncture is performed with a delayed inspiration in the 8th intercostal space along the mid-axillary line. When receiving blood from the needle, the Waldman apparatus is connected and the pressure is measured. In a healthy person, it is 150-200 mm. water. Art. With portal hypertension, the pressure can reach a level of more than 600 mm of water column.
Pressure increase over 300-350 mm of water. Art. is a risk factor for bleeding from varicose veins of the esophagus. The most dangerous complication of this method is intra-abdominal bleeding from the injured spleen. A contraindication is the patient's serious condition, pronounced activity of the pathological process in the liver, significant disturbances in the blood coagulation system and disorders of the renal excretory function.
- Measurement of the level of wedged hepato-venous pressure in the portal vein system and its branches
The value of the determined wedged posthepatic venous pressure (PVP) corresponds to the sinusoidal pressure. To determine sinusoidal pressure, a cardiac catheter is passed through the ulnar vein, the right heart and the inferior vena cava into one of the hepatic veins until the small diameter intrahepatic vein is jammed. Intra-splenic pressure (IRP) and free portal pressure (SPP) are also measured.
VSD is determined by puncture of the spleen and reflects the presinusoidal pressure. The same pressure reflects SPP, which is determined by catheterization of the mesenteric vein or the main trunk of the portal vein. Normal IRR and SPD are 16-25 mm Hg. Art., ZPVD - 5.5 mm Hg.
- Laparoscopy
Laparoscopy is used in doubtful cases. It is important to identify the nature of pathological changes in the liver, take a biopsy; determine the severity of splenomegaly and the degree of varicose veins of the portal system; establish the presence of ascites.
- Magnetic resonance imaging
- Additional examination methods
Additional examination methods are carried out in order to establish the etiological factor in the development of liver cirrhosis.
It is possible to diagnose hereditary diseases (hemochromatosis, alpha1-antitrypsin deficiency, Wilson-Konovalov disease, cystic fibrosis) that can cause liver cirrhosis.
- Taking anamnesis
- The goals of diagnosing portal hypertension
- Treatment of portal hypertension
Therapeutic measures are aimed at the prevention and elimination of complications (bleeding, ascites), as well as the treatment of diseases that caused portal hypertension.
- Treatment goals for portal hypertension
- Treatment of diseases that cause portal hypertension.
- Prevention and treatment of complications.
- Objectives of the treatment of portal hypertension
- Decrease in portal pressure.
- Stopping bleeding from the veins of the esophagus.
- Compensation of blood loss and elimination of hypoxia.
- Impact on blood coagulation potential.
- Treatment of liver failure.
- Diet therapy
In patients with portal hypertension, due to an increase in blood circulation in the internal organs, there is an increase in cardiac output, a decrease in blood pressure, and hypervolemia. Therefore, the diet of these patients should be low in sodium.
A salt-free diet is also indicated for ascites. A low protein diet is recommended for patients at high risk of developing hepatic encephalopathy. When symptoms of encephalopathy appear, it is necessary to reduce the amount of protein to 30.0 g per day with an even distribution throughout the day. Read more: Nutritional therapy for ascites. Nutritional therapy for liver cirrhosis.
- Drug therapy for portal hypertension
- Pituitrin.
The action of pituitrin is based on the narrowing of the arterioles of the abdominal organs, which causes a decrease in hepatic blood flow and a decrease in portal pressure by 40-60%.
To reduce portal pressure, intravenous pituitrin is prescribed at a dose of 20 units per 200 ml of 5% glucose solution for 15-20 minutes, then 5-10 units every 30-40 minutes. The infusion is repeated every 4 hours.
- Terlipressin.
Terlipressin (Remestip) is a synthetic analogue of vasopressin with a delayed action. It can be given in combination with vasopressin, 1–2 mg for 4 hours. With repeated administration, the effect of the drug decreases. In case of arterial hypertension, the drug is not recommended to be prescribed.
- Nitrates.
Nitrates are venous and arterial vasodilators. They reduce the total peripheral resistance, leading to the deposition of blood in the peripheral vessels and a decrease in blood flow to the portal system.
Nitroglycerin is administered intravenously at 40-400 μg / min. It can also be prescribed under the tongue at 0.6 mg every 30 minutes. Reduces portal pressure by 30%. It is used alone and in combination with pituitrin.
When nitroglycerin is combined with vasopressin, a significant reduction in portal pressure can be achieved.
To reduce the phenomena of portal hypertension, isosorbide dinitrate (Kardiket, Nitrosorbide), isosorbide mononitrate (Mono Mac, Olikard) can also be prescribed.
- Beta-blockers.
To reduce the phenomena of portal hypertension, beta-blockers (propranolol (Anaprilin, Obzidan)) are prescribed at 20-40 mg per day for a long time (months, years).
When taking beta-blockers, the heart rate should decrease by 25% from the initial level. These drugs are able to reduce portal pressure by about 40%. The effect is achieved by reducing cardiac output and decreasing heart rate.
- Somatostatin.
Somatostatin affects the smooth muscles of the mesenteric vessels and increases the resistance in the arterioles of the internal organs, thereby reducing portal blood flow.
A synthetic analogue of somatostatin - octreotide (Octreotide solution for injection, Sandostatin) is prescribed in doses of 25-50 μg. The drug also has a selective effect on vascular smooth muscle and inhibits the release of vasodilating peptides.
- Diuretic therapy.
Spironolactone (Veroshpiron) is prescribed 200-400 mg per day in combination with furosemide (Lasix) - 40-240 mg per day against the background of a salt-free diet.
Sometimes prednisolone (Prednisolone tablets) is prescribed 20-25 mg per day.
- Lactulose.
Lactulose (Duphalac, Normase) in the form of a syrup is taken at 30 mg 3-5 times a day after meals until a laxative effect appears. The drug creates an acidic environment in the colon, binds and reduces the formation of ammonia and aromatic amino acids in the intestine with cerebrotoxic effects. In the presence of constipation, it is advisable to cleanse enemas in a solution of magnesium sulfate.
- Antibacterial therapy.
It must be remembered that all patients with cirrhosis of the liver and bleeding from varicose veins of the esophagus and stomach have a high probability of developing bacterial infections.
Prophylactic antibiotics can reduce this risk. Until the identification of the pathogen, cefotaxime (Claforan, Cefotaxime por.d / in.) Can be administered intravenously 1.0 g 3 r / day.
- Pituitrin.
- Surgical treatment of portal hypertension
Indications for surgical treatment of patients with portal hypertension syndrome are: the presence of varicose veins of the esophagus or cardiac stomach with or without bleeding, splenomegaly with hypersplenism and ascites.
For patients with chronic liver diseases, a scoring scale (Child-Turcotte-Pugh scale) was developed for the severity of the disease, the risk during surgery, and the prognosis based on clinical and laboratory data.
- Child-Turcotte-Pugh Scale
Clinical and laboratory data Points 1 2 3 Hepatic encephalopathy (stages **) 1-2 3-4 Ascites Mild (or diuretic-controlled) Moderate despite taking diuretics Prothrombin time (sec.) < 4 >4-6 > 6 INR (International Normalized Ratio) < 1,7 >1,7-2,3 >2,3 Albumin (g / dl) >3,5 >2,8-3,5 < 2,8 Bilirubin (mg / dl) < 2 >2-3 >3 - 5-6 points - grade A (very low risk).
- 7-9 points - degree B (medium risk).
- 10-15 points - degree C (very high risk).
- Surgical methods for portal hypertension
- Portosystemic shunting
In portosystemic shunting, portocaval (general decompression) or distal splenorenal shunting is performed.
Bypass grafts are performed in patients with severity class A. Patients with severity class B are shown transjugular intrahepatic portosystemic bypass grafting.

- Devascularization of the lower esophagus and upper stomach (Sugiura operation)
Operation Sigiura involves:
- The transection of the esophagus and the imposition of reanastomosis with a circular suture using a stapler.
- Devascularization of the esophagus and stomach (ligation of the branches of the left gastric and short arteries and veins of the stomach, as well as subphrenic veins).
- Splenectomy.
- Stem vagotomy.
- Pyloroplasty.
The disadvantages of the operation include its high invasiveness.

- Portosystemic shunting
- Child-Turcotte-Pugh Scale
- Treatment of complications of portal hypertension
- Treatment of bleeding from varicose veins
The mortality rate of patients with each episode of bleeding from varicose veins is 30%. This complication occurs in patients with severe chronic liver disease and in patients who have already had episodes of bleeding. Rebleeding occurs in 40% of patients within 6 weeks after the first episode.
The general condition of the patient and the functional state of the liver affect the effectiveness of treatment of bleeding from varicose veins of the esophagus and stomach.
Surgical intervention with ongoing bleeding from the cardiac stomach and lower esophagus should be performed as soon as possible in patients in groups A and B according to the Child-Pugh scale. In patients of group C on the Child-Pugh scale, surgery is associated with a high risk of complications and mortality.
With the ineffectiveness of therapy with beta-blockers, as a forced measure, they resort to surgical intervention (ligation of varicose veins with rubber rings or bypass surgery).
Portosystemic shunting or esophageal closure of veins is performed if there is a history of recurrent bleeding. As a rule, these are patients with prehepatic portal hypertension, which is characterized by the early development of ascites that does not respond to diuretic therapy, accompanied by pain in the liver area, significant splenomegaly.
Stopping the resulting bleeding from varicose veins of the esophagus is carried out against the background of replenishing blood loss (plasma substitutes, erythromass, donor blood, plasma) in combination with the introduction of vicasol, calcium chloride.
- Endoscopic sclerotherapy
Sclerotherapy of dilated veins may be more effective than prescribing beta-blockers (propranolol (Anaprilin, Obzidan)) to prevent bleeding, but it has more side effects.
Endoscopic sclerotherapy is used at the height of bleeding, immediately after stopping bleeding, in identifying risk factors for bleeding (varicose veins of II-III degree, the value of portal pressure more than 300 mm H2O, the appearance of red markers on the esophageal mucosa).
The serum can be administered in two ways: intra- and perivasally. In the first method, a sclerosing drug is injected through an endoscope (using a catheter - a needle in a volume of 2-8 ml) into a varicose vein of the esophagus in order to develop thrombosis in it. In case of unstable hemostasis, a Blackmore tube is placed in the esophagus.
With the perivasal method, the sclerosant is injected into the submucosal layer around the vein. The effect in this case is achieved due to the development of edema of the submucosal layer, followed by perivasal fibrosis. The first method is preferable for large, the second - for small varicose veins.
The following sclerosing agents are most often used: 5% solution of ethanolamine oleate (Etamolin), 1-3% solution of polidocanol (Ethoxysclerol), 3% sodium tetradecyl sulfate solution (Fibro-Wayne, Thrombovar) for paravasal administration.
The advantages of this method are: the possibility of selective obliteration of the veins of the esophagus and the cardiac part of the stomach in those places where their risk of rupture is maximum; no negative effect of the procedure on liver function and low invasiveness of the method. The method allows to stop bleeding in 70% of patients.
Complications of sclerotherapy: necrosis of the esophageal wall when sclerosant enters the muscle layer of the esophagus, ulceration of the mucous membrane of varying severity.
Endoscopic sclerotherapy as an independent method of treatment is indicated for patients with a high risk of surgery, in whom conservative therapy was ineffective, as well as for patients who have been repeatedly operated on for bleeding from esophageal varicose veins.

- Endoscopic sclerotherapy
- Treatment of splenomegaly and hypersplenism
One of the manifestations of portal hypertension is splenomegaly and hypersplenism (erythropenia, leukopenia, thrombocytopenia).
To increase the number of leukocytes in hypersplenism, leukopoiesis stimulants are prescribed for 1-3 months.
In the absence of effect, prednisolone is prescribed (Prednisolone table) in doses of 20-40 mg for 2-3 months. Erythrocyte and platelet masses are transfused.
- Splenectomy
Splenectomy reduces portal pressure, including esophageal veins, but as an independent operation it is not decisive. Splenomegaly without signs of cytopenia is subject to surgical treatment only if the spleen of a very large size compresses the abdominal organs, disrupting their function.
Splenomegaly with severe hypersplenism and hemorrhagic syndrome is a direct indication for splenectomy. In the postoperative period, severe complications such as thrombocytosis and hemorrhagic thrombocytopenia may develop.
- Splenic artery embolization
This method of treatment for hypersplenism reduces portal pressure, relieves the phenomenon of hypersplenism and allows in the future to perform, if necessary, more complex repeated corrective operations.
- Splenectomy
- Ascites treatment
Patients with ascites are prescribed spironolactone (Veroshpiron), 100-150 mg daily. In the absence of effect, it is advisable to use furosemide (Lasix) 40-80 mg 2-3 times a week.
With ascites, hypoalbuminemia is usually observed, which also contributes to the development of ascites. To correct it, they are prescribed intravenously: 100 ml of albumin, 400 ml of fresh frozen plasma in 1-2 days.
With ascites resistant to conservative therapy, surgical interventions are performed designed to drain ascites fluid. Read more: Treatment of ascites.
- Hepatic encephalopathy treatment
In order to reduce the content of ammonia in the blood, it is necessary to reduce the amount of protein in the diet (up to 20-30 g per day); a vegetable and vegetable diet is recommended; enemas or the use of laxatives to cleanse the intestines. It is important to have a bowel movement at least 2 times a day.
For this purpose, Lactulose (Duphalac, Normase) is prescribed, 30-50 ml orally every hour until diarrhea appears, then 15-30 ml 3-4 times a day. For use in an enema, 300 ml of the drug's syrup are diluted in 700 ml of water and all parts of the large intestine are filled.
Antibacterial therapy is used: neomycin 1 g orally 2 times a day, metronidazole (Trichopolum, Flagil) 250 mg orally 3 times a day or vancomycin (Vancocin) 1 g orally 2 times a day.
Liver transplantation indicated.
- Treatment of bleeding from varicose veins
- Treatment goals for portal hypertension

- Prognosis for portal hypertension
The prognosis in patients with portal hypertension is determined by the presence of bleeding and the severity of liver dysfunction.
The risk of recurrent bleeding from varicose veins within 1–2 years after the first episode is 50–75%.
10097 0
TREATMENT STRATEGY
Varicose veins of the esophagus and stomach with relapses or the threat of bleeding from them are considered the main complication of portal hypertension, requiring active (most often surgical) treatment, since each recurrence of gastroesophageal bleeding, in addition to the immediate threat to the patient's life, leads to a significant deterioration in liver function, often to the development of liver failure, encephalopathy and ascites.Currently, there are three principal approaches to the prevention and prevention of bleeding from varicose veins of the esophagus and stomach.
The first - involves decompression of the portal system using portocaval shunting. For this purpose, various types of vascular portocaval anastomoses are used, including transjugular portosystemic shunting ( transjugular intrahepatic portosystemic shunt - TIPS).
Second approach consists in the separation of the portocaval connections in the area of \u200b\u200bthe esophageal and gastric varicose veins using various surgical operations. This can be devascularization of the esophagus and stomach, transection of the esophagus, suturing and ligation of veins in the esophagocardial region, resection of the esophagus and stomach, as well as "minimally invasive" interventions: endoscopic sclerotherapy or ligation of varicose veins, endovascular embolization of the left gastric vein and short veins of the stomach. The purpose of these operations is to interrupt the blood flow to and through the veins in the cardioesophageal region.
Third - consists in reducing portal pressure with drugs. At the same time, it is assumed to maintain a significant pressure gradient between the portal and caval systems.
All of these treatments are palliative: they are aimed not at treating the underlying disease, but at eliminating one of the main symptoms of portal hypertension - bleeding from varicose veins of the esophagus and stomach. The only radical treatment for hypertension in the portal vein system in patients with decompensated liver cirrhosis is liver transplantation.
MEDICINE TREATMENT
Drug prevention of bleeding from varicose veins of the esophagus and stomachCurrently for the prevention of bleeding from varicose veins of the esophagus and stomach in patients with liver cirrhosis, non-selective β-blockers are used: propranolol, anaprilin, nodolol, etc. These drugs lead to a decrease in portal pressure due to a decrease in cardiac output and a decrease in pulse rate. Bradycardia reduces portal pressure by 25% and reduces the risk of bleeding by 20-30%. The dose of the drug is selected individually. Combined use of β-blockers and nitrates is possible. If there are contraindications to the use of β-blockers, long-acting nitrates are used to reduce portal pressure. In patients with extrahepatic hypertension, such prophylaxis is not performed.
SURGERY
Bleeding from varicose veins of the esophagus and stomach is the main cause of death in patients with portal hypertension, therefore, the treatment and prevention of this manifestation of the disease is the main indication for surgical intervention.In patients with liver cirrhosis, prophylactic surgical treatment is indicated only when there is a clear threat of bleeding, i.e. with varicose veins of the esophagus and stomach II-III degree with symptoms of vasculopathy and esophagitis. In patients with grade I and II varicose veins, but without disorders of the trophism of the mucous membrane, surgical treatment is not performed. Such patients are observed with annual endoscopic control.
In extrahepatic portal hypertension, the indications for prophylactic surgical treatment may be broader, since successful portocaval shunting leads to recovery in these patients, and the likelihood of technical performance of shunting operations for this pathology is higher at a young age, in the early stages of the pathological process.
Resistant ascites in portal hypertension can also be considered an indication for surgical treatment, since the quality of life of these patients is extremely low, and further conservative treatment is futile. Since in most cases persistent ascites is a sign of liver cirrhosis decompensation, the risk of performing major operations is extremely high. The advantage is given to palliative surgical interventions that make life easier for these patients.
The selection of patients with hypertension in the portal vein system for performing various surgical procedures is a very crucial moment. Patients with extrahepatic portal hypertension rarely require special preoperative preparation, due to the preservation of the functional ability of the liver. However, with hypertension secondary to diseases of the blood system or thrombophilia, there is a high risk of thrombotic or hematological complications, which must be taken into account in preoperative preparation. In such situations, it is carried out in conjunction with hematologists (cytostatic therapy for myeloproliferative diseases and anticoagulant therapy for the prevention of thrombotic complications).
Another clinical situation in patients with liver cirrhosis and portal hypertension. The choice of an appropriate surgical aid and prediction of the results of surgical treatment for such patients are closely related to a more accurate objectification of the depth of the lesion of the hepatic parenchyma, an assessment of the reserve capacities of the liver and the body as a whole. Despite certain shortcomings, the Child-Pugh predictive test system (see above) is considered the most practical and convenient. Its disadvantage is the underestimation of the nutritional status criterion and the arbitrary nature of the scoring system used. When deciding on a surgical intervention, in addition to the Child-Pugh criteria, the activity of the process should be determined according to the data of the main cytolysis enzymes (ACT, ALT), the severity of cholestasis and the state of the parameters of central hemodynamics.
Adhering to the Child-Pugh classification, most researchers consider it possible and advisable to use a surgical method of treatment in patients with functional classes A and B. With decompensated cirrhosis of the liver (class C), the risk of surgery is extremely high, and in the event of bleeding from varicose veins, the advantage is given to minimally invasive or conservative methods of treatment.
PREOPERATIVE PREPARATION
Preoperative preparation of patients with portal hypertension in liver cirrhosis includes the normalization of the functions of the affected organ, improvement of metabolic processes, reduction or elimination of the severity of clinical manifestations of the main symptoms of the disease. The complex of therapeutic measures consists of general and specialized methods of therapy.General directions of treatment:
... infusion-blood transfusion therapy with transfusion of blood products (albumin, plasma, erythrocyte mass), glucose-saline solutions, aimed at correcting metabolic disorders and anemia;
... cardiac therapy for signs of heart failure;
... vitamin therapy (group B drugs);
... local and general therapy of inflammatory lesions of the mucous membrane of the esophagus and stomach;
... a short course of hormone therapy with an active process in the liver (intravenously: prednisolone 150-200 mg / day, followed by a dose reduction within a week to 30 mg).
Specialized methods of preoperative preparation:
... diuretic therapy under the control of water balance for edematous-ascites syndrome;
... drug prevention of the threat of bleeding from varicose veins (β-blockers, nitrates);
... treatment of latent or clinically overt hepatic encephalopathy (lactulose preparations, intravenous or oral ornithine);
... antioxidant therapy;
... Nutrient-metabolic therapy aimed at correcting protein-energy malnutrition and the most important metabolic disorders.
The specific nature of nutrient-metabolic therapy is associated with the need to use a source of amino nitrogen, in which the proportion of aromatic amino acids (phenylalanine, tyrosine, and tryptophan) is reduced and the content of branched-chain amino acids (leucine, isoleucine, valine) is increased. For parenteral nutrition, metabolically adapted amino acid mixtures are used, such as 5 and 8% aminosteril-Hepa solution or 10% aminoplasmal-Hepa solution. For the treatment of hepato-portal encephalopathy, parenteral amino acid compositions can be used: ornithine. For the purpose of enteral probe correction of metabolic disorders, Hepatonutril (Spain), Falkamin (Germany), Nutricom-hepa (Germany), Nutrigep (CIIIA), Fresubin-Hepa (Germany), as well as domestic the remedy is hepencefamine.
While maintaining the possibility of feeding through the mouth or when switching from tube to oral nutrition, specialized protein-amino acid modules are used as a supplement to natural food products: Hepamin, Lactostrict (Germany), containing minerals, trace elements and vitamins.
Decreased tolerance to protein load and the presence of signs of latent or shunt encephalopathy require the appointment, in addition to the diet, of specialized protein-amino acid modules "Hepamin-Special" (Russia) or "Falkamin Pellets" (Germany). This treatment can be supplemented with oral ornithine or lactulose preparations.
If, as a result of preoperative preparation, a noticeable therapeutic effect is not obtained, the reserve capabilities of the patient with liver cirrhosis should be reassessed and correlated with the risk of the planned operation. If you have any doubts about the tolerance of the proposed surgical intervention, you should abandon the planned operation in favor of a less traumatic treatment and continue corrective therapy.
A.K. Eramishantsev, A.G. Scherzinger, E.A. Kitsenko
Portal hypertension: symptoms
Pathology can lead to the development of life-threatening complications, such as enlargement of the veins of the stomach, rectum, esophagus. When the veins in the lumen stretch, their walls become thinner, which can rupture and, as a result, cause bleeding (internal or external). Often, patients with varicose veins have bloody, tarry black stools. Portal hypertension often leads to encephalopathy. The complication occurs because the damaged liver cannot remove toxins from the blood. They enter the brain, cause disturbances in its functioning and damage nerve cells. In the presence of encephalopathy, patients have forgetfulness and lethargy. Also, portal hypertension can cause ascites, which is characterized by the accumulation of fluid in the abdominal cavity due to very high pressure in the portal vein. Patients suffering from this ailment observe symptoms such as an increase in the volume of the abdomen and pain in it. Loss of appetite is also noted as a result of fluid pressure on the stomach and shortness of breath as a result of its effect on the lungs. Sometimes ankle swelling may occur.

Portal hypertension: diagnosis
If portal hypertension is suspected, the doctor will most likely perform an upper GI endoscopy to confirm the diagnosis. During the procedure, a thin tube with a camera (endoscope) is inserted into the stomach and duodenum through the esophagus. In this way, the doctor can see the condition of the organs, as well as take a tissue sample for a biopsy. In addition to endoscopy, ultrasound diagnostics can also be performed.
Portal hypertension: treatment

The pathology is most often treated surgically - through a transjugular intrahepatic portosystemic shunt - an operation in which the doctor makes a small incision in the portal vein and inserts a small tube into it. It is connected to one of the liver veins, thereby creating an additional pathway for blood flow. Such an operation can reduce pressure in all the veins of the abdomen, including the esophagus, intestines and stomach. However, before this procedure is carried out, the patient must undergo many studies aimed at studying the work of the heart and the pressure in the portal system of the liver. Such studies include, in addition to endoscopy and ultrasound diagnostics, which have already been mentioned, also echography of the heart and blood tests. Portal hypertension is also treated with sclerotherapy, where a doctor injects a special fluid into a vein to cause scarring. The use of this method does not lead to a decrease in pressure, but strengthens the shell of the vessels, which allows them not to pass liquid and not to rupture. Sclerotherapy is carried out only when it is impossible to carry out banding - a procedure that involves ligating blood vessels and slowing blood flow.
This is an increase in pressure in the portal vein system, which occurs when blood flow in the portal vessels, hepatic veins and inferior vena cava is disturbed.
Through the portal vein, the bulk of the blood from the abdominal organs enters the liver. This is more than 75% of all blood that goes to the liver. The liver receives the remaining 25% of the blood through the hepatic artery. The human body has natural portocaval anastomoses in the areas of the rectal and gastroesophageal venous plexuses. There are also natural portocaval anastomoses and anastomoses in the umbilical vein system, which connect to the veins of the abdominal wall and diaphragm. Three more groups of anastomoses are located in the retroperitoneal tissue:
- between the veins of the mesentery and kidneys;
- between the superior mesenteric and splenic veins;
- between the splenic and left renal veins.
¾ hepatic capillaries do not function, they constitute a reserve of intrahepatic blood flow. From the liver, blood flows through the hepatic veins, which flow into the subphrenic part of the inferior vena cava. Inside the liver, between the hepatic and portal veins, portocaval anastomoses are formed. At the heart of the pathogenesis of portal hypertension is the obstruction of blood flow by the portal vein system. Usually this block is mechanical, but there are cases of functional (spastic) blockage of portal blood flow.
There are the following types of portal blood flow blockade:
- intrahepatic (found most often);
- prehepatic;
- suprahepatic;
- mixed (thrombosis of the portal vein or its branches occurs).
Each of the forms is characterized by the localization of the blocked vessel.
Early signs include:
- persistent dyspeptic symptoms, especially after eating: bloating after eating any food;
- feeling of constantly full bowel without pronounced constipation;
- progressive weight loss and hypovitaminosis with preserved appetite and virtually normal energy value of food;
- periodically painless and temperatureless diarrhea.
Patients complain of increased fatigue, decreased performance, recurrent pain in the epigastric region, bleeding from the nose, gums, and later gastroesophageal bleeding occurs.
Portal hypertension symptoms:
- dyspeptic symptoms (nausea, flatulence, unstable stool, etc.)
- expansion of the saphenous veins in the abdomen
- edema
- jaundice (rare)
- ascites
- gastrointestinal bleeding
- enlarged spleen
- exhaustion
How is portal hypertension treated?
It is aimed primarily at the underlying disease and at preventing complications. To reduce pressure, antihypertensive drugs and diuretics are prescribed. Antibiotic therapy is also recommended to prevent the development of bacterial infections. In addition, hormonal drugs can be prescribed to regulate the work of vascular smooth muscles. Taking lactulose preparations stimulates the intestines, sometimes cleansing enemas are indicated. In the event of bleeding, hemostatic drugs may be additionally prescribed along with nitrates.
Diuretics are ineffective in this case, which is a poor prognostic sign. If thrombophlebitis of the veins of the portal system (pylephlebitis) develops, fever appears, which lasts a long time and is accompanied by episodes of esophagogastric bleeding.
Treatment of portal hypertension should be comprehensive - conservative and surgical. To reduce portal hypertension, somatostatin (stylamine) is administered intravenously (3000 mg for 12-24 hours), which is effective in 90% of cases, then propranolod (40-80 mg) is used for a long time.
Surgical treatment of portal hypertension is performed in two cases:
- in urgent order at the height of acute profuse bleeding in order to stop it;
- in a planned manner to sustainably reduce pressure in the portal system and eliminate ascites and hypersplenism.
Indications for surgical treatment are bleeding that does not stop with conservative therapy, ascites, an enlarged spleen, and persistent bleeding. Depending on the complication that has arisen, the method of surgical intervention is selected.
In urgent conditions with diffuse esophagogastric bleeding, esophageal tamponade is effective, including transesophageal tamponade with the help of esophagoscopy, administration of sclerosing 66% glucose solution into varicose veins, posterior mediastinotomy with mediastinal tamponade, methods of devascularization of the cardiac part of the stomach, abdominal, etc. Of the planned surgical methods, splenorenal anastomosis with removal of the spleen deserves attention, which eliminates not only portal hypertension, but also the phenomenon of hypersplenism.
In the arsenal of the surgeon, there are other methods of treating portal hypertension (portocaval, mesenteric-caval, cavomesenteric anastomoses, etc.).
What diseases can be associated with
In the development of portal hypertension of intrahepatic origin, the most important are:
- in the liver,
- congenital narrowing of the portal vein,
- anomalies of intrahepatic branching of the portal vein.
The prehepatic form of portal hypertension is caused by:
- portal vein trunk,
- cavernous transformation of the portal vein trunk,
- congenital obliteration or stenosis of the portal vein,
- compression of the portal vein
- tumor
- scars,
- infiltrates,
- lymph nodes
- primary or secondary portal cytosclerosis,
- or ,
- splenic or hepatic.
The cause of the suprahepatic block is often difficult to establish. In the development of the syndrome of suprahepatic portal hypertension, the most important are:
- hepatic vein thrombosis (),
- compression of the hepatic veins or the trunk of the inferior vena cava with a scar or tumor,
- right ventricular heart failure,
- squeezing.
Portal hypertension, and with it, usually aggravate such pathology as cirrhosis of the liver.
Treatment of portal hypertension at home
Treatment of portal hypertension it is impossible to carry out at home. Since there is a constant risk of bleeding, treatment should be carried out in a hospital under the constant supervision of doctors.
What are the drugs to treat portal hypertension?
- Pituitrin
Treatment of portal hypertension with alternative methods
Treatment of portal hypertension with the help of folk recipes is ineffective, since this is an acute condition that requires hospital treatment.
Treatment of portal hypertension during pregnancy
Pregnancy is a contraindication for the diagnosis of portal hypertension. Therefore, the decision to continue the pregnancy is made by the attending physician, after assessing all the risks for the woman and the child.
Which doctors should you contact if you have portal hypertension
Methods for detecting portal hypertension:
- X-ray examination of the esophagus and the cardiac part of the stomach in order to identify varicose veins; this method makes it possible to verify varicose veins in 16-18% of patients. Now they use computed and nuclear magnetic resonance imaging.
- Esophagoscopy - shows varicose veins of the esophagus in 69% of patients. The percentage of positive results increases if, during an esophagoscopy, the patient is in the Trendelenburg position.
- Sigmoidoscopy - allows you to see varicose veins, the diameter of which reaches 4-6 mm.
- Portohepatomanometry - performed by puncture of the liver in the ninth to tenth intercostal spaces along the middle axillary line on the right.
- Splenomanometry - spleen puncture is performed in the ninth to tenth intercostal spaces along the middle or posterior axillary lines on the left. The puncture needle is connected to a manometer, normally the internal-splenic pressure is 120-180 mm of water. Art. Pressure increase over 200 mm of water. Art. indicates a violation of the portal circulation. In patients with an intrahepatic portal vein block, the level of splenic pressure is a likely criterion for pressure in the portal vein system.
- Splenoportography is an X-ray method for examining the portal circulation. Through a puncture needle, 20-40 ml of a radiopaque substance (urotrast, cardiotrast, diodon) is injected into the spleen. Serial images are taken (after 1, 3, 5, 7, 9 and 11 sec.). Establish the patency of the splenoportal bed, branching of the portal vein in the liver, the presence of venous reflux, and the like.
- Laparoscopy with puncture biopsy - helps to establish the degree of liver damage, to identify enlarged veins of the omentum, stomach, visual morphological changes in the liver.
The main clinical sign of suprahepatic portal hypertension is splenomegaly without ascites and bleeding from dilated esophageal veins. More often splenomegaly is accompanied by hypersplekism. Then the triad is determined: hypersplenism, bleeding, ascites.
The liver is usually not palpable. Portal hypertension develops slowly. In case of bleeding, the course worsens - ascites and signs of hepatic cell failure appear. The most striking signs of intrahepatic portal hypertension are splenomegaly, varicose veins of the esophagus with possible bleeding, ascites.
The surface of the liver is unevenly bumpy. Sometimes the liver is very reduced in size. The spleen is usually enlarged. Bleeding from hemorrhoidal veins is often non-massive. Itching of the skin often appears long before jaundice. On it, spider veins on the palms are found - erythema. In men - gynecomastia and impotence, in women - amenorrhea, atrophy of the mammary glands. A hypersplenic triad is determined in the blood: anemia, leukopenia, thrombocytopenia.
Treatment of other diseases with the letter - p
| Pancreatitis treatment |
| Pancreatic necrosis treatment |
| Treatment of papilloma of the trachea |
| Parametritis treatment |
| Treatment of paraneoplasias |
| Paranephritis treatment |
| Head lice treatment |
| Pelvioperitonitis treatment |
| Testicular torsion treatment |
| Patella fracture treatment |
| Treatment of periarthritis of the shoulder joint |
| Pericarditis treatment |
| Hepatic coma treatment |
A disease such as portal hypertension refers to a syndrome that occurs as a result of impaired blood flow in combination with an increase in blood pressure in the portal vein. Portal hypertension, the symptoms of which are based on manifestations characteristic of dyspepsia, ascites, splenomegaly, varicose veins of the stomach and esophagus, as well as gastrointestinal bleeding, as a radical method of treatment requires surgical intervention.
general description
In addition to the fact that portal hypertension has an extensive complex of symptoms caused by increased blood pressure of the portal vein bed (a large vein through which blood flows from the intestine to the liver) with a simultaneous violation of venous blood flow, characterized by different etiology and concentration, this disease can also act as a factor complicating another kind of disease. In particular, portal hypertension can provoke their complications in hematology, vascular surgery, gastroenterology and cardiology.
The development of portal hypertension is also possible as a result of pathologies caused (extrahepatic or intrahepatic form). In addition, the development of this disease is facilitated by primary / secondary biliary cirrhosis, tumor of the bile hepatic duct, tumor of the common bile duct, ligation or intraoperative damage to the bile ducts. A certain role in the development of the disease in question is also assigned to the toxic damage to which the liver is exposed as a result of poisoning with hepatotropic poisons (mushrooms, medications, etc.).
Allocate in the development of portal hypertension and such pathological processes in the body as a congenital form of atresia and, stenosis or tumor compression, concentrated directly in the area of \u200b\u200bthe portal vein, increased pressure of the right heart (current pathology in constrictive pericarditis and restrictive cardiomyopathy). Sometimes portal hypertension develops as a result of processes that have arisen against the background of critical conditions - with injuries, operations and burns on a large scale.
Infections and therapy of a massive nature based on the intake of diuretics and tranquilizers, bleeding in the gastrointestinal tract, an excess of animal proteins in the diet and the abuse of alcoholic beverages are often determined as decisive factors acting in the form of a kind of impetus in the formation of the clinical picture of the disease. A feature of the mechanism of the disease we are considering is an increase in hydromechanical resistance. In general, the features of the origin of portal hypertension, as well as the features of its development, have not been sufficiently studied to date.
Features of the course of portal hypertension
Portal hypertension in its own course can correspond to the functional stage and the organic stage. The functional stage is characterized by the tone characteristic of peripheral vessels, the regulatory features of the liver blood flow, as well as the rheological vessels of the portal system. As for the organic stage, it is characterized by the compression of sinusoids and their destruction, the appearance of portohepatic vessels and the proliferation of connective tissue in the lobar centrilobular zones. Let's highlight the main processes that characterize the pathology of interest to us in general:
- the occurrence of a mechanical obstacle that interferes with the outflow of blood;
- increased blood flow in the portal veins;
- increased resistance from the portal vessels;
- the formation of collaterals between the systemic blood flow and the portal vein bed;
- the development of ascites, which is one of the most important symptoms of the disease;
- splenomegaly (that is, enlargement of the spleen), arising as a consequence of portal hypertension and characterized by stagnation in combination with cell hyperplasia in the reticulo-histiocytic system and proliferation of connective tissue in the spleen;
- - the state into which portal hypertension passes with the development of porto-caval anastomoses.
Portal hypertension: classification
Based on the degree of prevalence characteristic of the zone in which there is an increase in blood pressure, the portal bed may have total portal hypertension or segmental hypertension. In the first case, the disease covers the vasculature that belongs to the portal system completely, in the second case, there is a corresponding restriction of blood flow disturbance along the splenic vein while maintaining normal pressure and blood flow in the mesenteric and portal veins in this process.
In accordance with the localization characteristic of the venous block, prehepatic and intrahepatic portal hypertension, as well as mixed hypertension, are determined. The difference in the forms of the disease suggests the presence of its own causes that contribute to their occurrence. For example, prehepatic portal hypertension, noted in about 4% of cases, is formed as a result of impaired blood flow in the splenic and portal veins, which is explained by their compression, thrombosis, stenosis and other pathological manifestations, etc.
The structure of the intrahepatic form of the disease can have presinusoidal, sinusoidal and postsinusoidal blocks. In the first variant, the interfering factor is in front of the sinusoids (in the case of polycystic disease, schistosomiasis, sarcoidosis, tumor and nodular hepatic transformations), in the second - in the hepatic sinusoids (cirrhosis, tumors, hepatitis), in the third - beyond the alcoholic sinusoids (fibrosis, disease, cirrhosis of the liver, veno-occlusive disease).
Subhepatic portal hypertension, noted in about 12% of cases, is due to the urgency of Budd-Chiari syndrome, compression or thrombosis of the inferior vena cava, constrictive pericarditis, or other reasons.
Based on the previously listed processes inherent in pathology and the corresponding features of symptoms, the following stages are distinguished:
- functional stage (initial);
- compensated stage (moderate) - splenomegaly is characterized by moderate manifestations, no ascites, the veins of the esophagus are subject to slight expansion;
- decompensated stage (pronounced) - splenomegaly, edematous-ascitic and hemorrhagic syndromes have a pronounced character of manifestations;
- portal hypertension with complications - in particular, bleeding arising from varicose veins of the stomach, esophagus and rectum, as well as manifestations in the form of liver failure and spontaneous peritonitis, are isolated as the latter.
Portal hypertension: symptoms
The earliest symptoms of portal hypertension are dyspeptic in nature, which, accordingly, is expressed in such manifestations as flatulence, nausea, unstable stool (constipation, diarrhea), a feeling of fullness in the stomach, pain in the epigastric, iliac and right hypochondrium regions. There is also a loss of appetite and the appearance of weakness, the patient dramatically loses weight and quickly gets tired, in addition to this, jaundice develops.
In some cases, splenomegaly is the main symptom that manifests itself among the first symptoms of the disease, and the degree of its severity is determined by the characteristics of the level of obstruction in combination with the magnitude of the pressure that characterizes the portal system. After the bleeding in the gastrointestinal tract is completed, the spleen decreases in size, which is also facilitated by a decrease in pressure that is relevant for the portal system in the generality of the processes under consideration.
A combination of splenomegaly and hypersplenism is also possible, which is a syndrome, the main manifestations of which are leukopenia, etc. The development of this syndrome is facilitated by an increased level of destruction of formed elements in the blood of the spleen when they are partially deposited (that is, they are temporarily disconnected from the processes of exchange and circulation during storage in the body for use after a while).
The difference between ascites in its course with the disease in question is the persistence of manifestation in it, as well as resistance in relation to the therapy applied to it. In addition to this, a symptom is noted in which the volume of the abdomen increases, the ankles are exposed to swelling. Examination of the abdomen reveals the presence of a network of dilated veins, concentrated in the area of \u200b\u200bthe abdominal wall, while in appearance this manifestation is similar to the "head of a jellyfish".
A rather dangerous and characteristic manifestation of portal hypertension is bleeding that occurs in the varicose veins of the stomach, esophagus, and rectum subject to changes under the influence of varicose veins. Bleeding in the gastrointestinal tract is of a sudden nature, while their distinctive feature is the abundance and tendency to recurrence.
Due to these features, the appearance of post-hemorrhagic anemia is quickly noted. In the event of bleeding from the stomach and esophagus in the case of the disease under consideration, melena appears (black stools of a tarry consistency, which has a fetid odor), as well as bloody vomiting.
Hemorrhoidal bleeding is characterized by the appearance of discharge from the rectum in the form of scarlet blood. It should be noted that bleeding that occurs with portal hypertension can be triggered by various mucosal injuries, decreased blood coagulability, increased intra-abdominal pressure and other factors.
Diagnosing portal hypertension
The methods for diagnosing the disease we are considering include the following:
- (determines the signs corresponding to hypersplenism: anemia, leukopenia, thrombocytopenia);
- (carried out for signs of liver damage);
- sigmoidoscopy (determines the visible presence of varicose veins in the area of \u200b\u200bthe sigmoid and rectum under the mucosa);
- esophagoscopy (allows you to identify the veins of the stomach and esophagus that have undergone varicose veins);
- (determines the possibility of assessing the diameter of the splenic and portal veins, and also allows you to identify the presence of collaterals and diagnose portal vein thrombosis);
- computed tomography and magnetic resonance imaging tomography (provides the ability to visualize the vessels of the liver);
- dopplerography (determines the speed inherent in portal blood flow);
- angiography (indicates the presence of masses in the liver);
- hepatomanometry , splenomanometry (determine intrahepatic pressure, as well as the degree inherent in the course of portal hypertension).
Treatment of portal hypertension
Antihypertensive drugs are used as a therapeutic measure aimed at reducing pressure in the portal vein.
The appearance of bleeding provides for the need for emergency care, which consists in the intravenous administration of drugs that reduce pressure (octreotide, vasopressin). In some cases, a blood transfusion is also required to replace the blood loss.
Stopping bleeding by endoscopic methods consists in the following actions:
- ligation of veins or injection to stop bleeding;
- insertion of a catheter equipped with a balloon at the end. Subsequently, it is inflated, which leads to compression of the varicose veins and, accordingly, to the cessation of bleeding.
Shunting is used as a surgical method of treatment. In this case, surgical intervention consists in creating a shunt (bypass) in the area between the portal system and the venous system. Due to this action, a decrease in pressure in the portal vein is ensured, because in the general venous system it is an order of magnitude lower. The bypass method is the most applicable in practice, however, there are a number of other surgical methods that also manifest themselves from a fairly effective side.
Portal hypertension: prognosis
From the moment of the first bleeding, mortality is about 40-70% of cases, while the surviving patients (the remaining 30%) subsequently die due to recurrent bleeding, which usually occurs within a period from several days to six months from the moment of its first episode.